


Hospitals Begin Testing for H5N1 Bird Flu
The threat has gotten serious enough that hospitals are now looking for the disease (When it makes sense clinically)

As you likely well know, H5N1 Highly Pathogenic Avian Influenza is becoming a scourge throughout animal populations across the United States and other countries. There has been crossover from wild and farm animals to humans, but as of yet no documented human to human transmission. That is the one relief we have for now.
But many hospital systems are now reflexively testing for H5N1 if there is a clinical history that suggests the disease could be at hand. This memo was sent at one of the large hospital systems I work at occasionally:
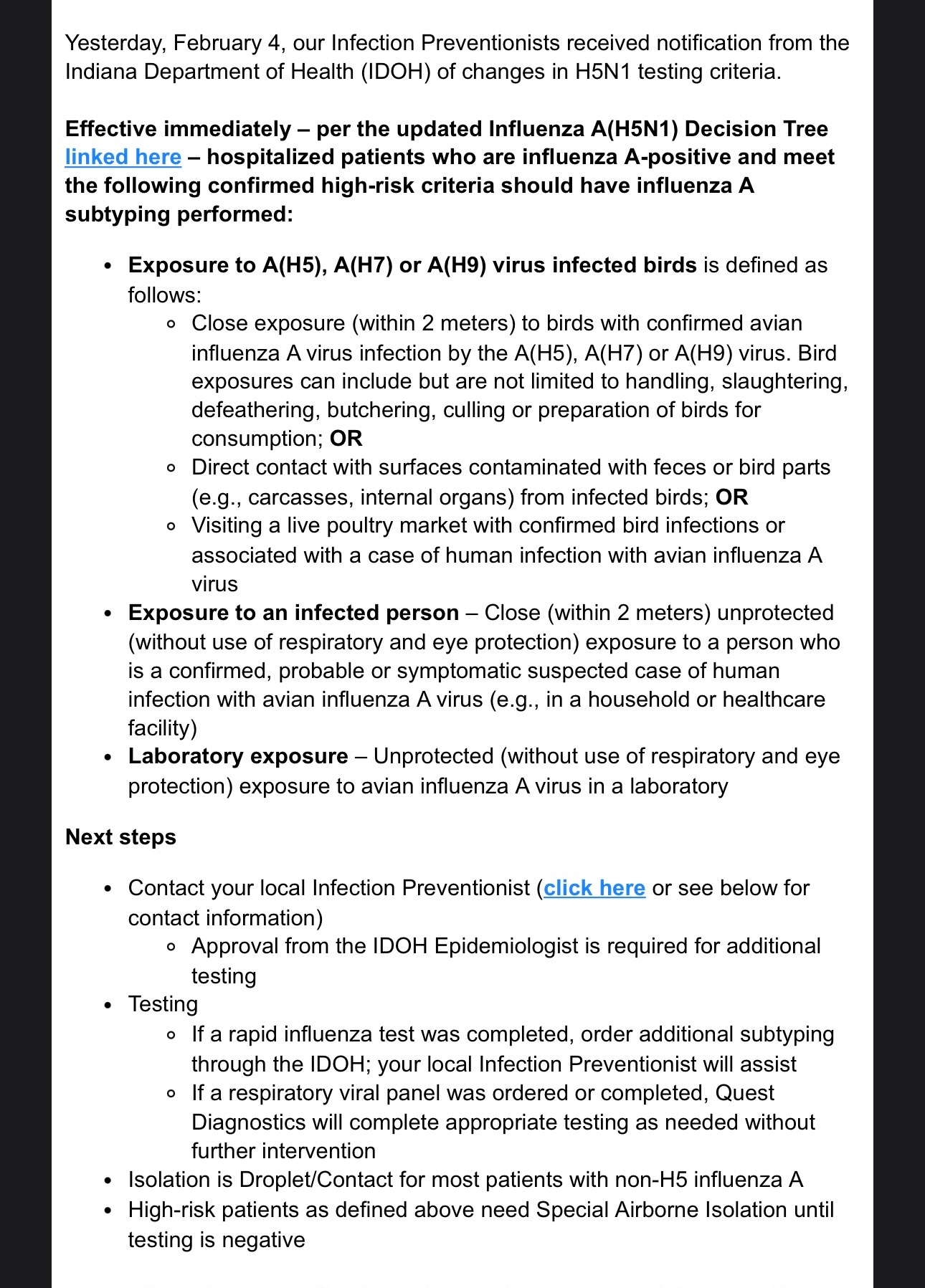
You’re welcomed to read the whole thing word for word, but in short, if a patient tests positive for influenza type A the decision to go ahead and look for H5N1 is based on whether or not that patient has close proximity to animals, a lab exposure, or close exposure to someone with known avian flu. Flu A is by far the most common type circulating right now, and the subtype is based on the surface proteins hemagglutinin and neuraminidase. Those proteins are how we subtype flu. Swine flu for instance is H1N1, and there are other types such as H3N2 and there was even an H9 circulating recently.
I recently had a case where a family wanted an autopsy on their loved one who passed and she had tested positive for influenza A. My first question? “Do you live on a farm?” Remarkably, the answer was “yes”. Unremarkably, I live in Indiana so most of the population either lives on a farm or is farm-adjacent. I asked if they had seen or handled any dead animals—I was already mentally screening for bird flu. The man said they had not. Ultimately, he decided he no longer wanted an autopsy so we cannot be certain exactly what H/N this infection was. But suffice it to say her clinical course was swift enough to make me think of it.
The moral is…this is the mode of thinking that we have to do now. To properly detect, to have a sensitive detection system in our communities, we need to be thinking “worst case scenario”. I don’t know how reliable our government will be in alerting us to critical information going forward, so we must aggregate the experiences and observations of what is happening in our communities and report them publicly. Stay vigilant! Stay alert!
—DLW
ebruary 3, 2025
TO: FROM: Hospitals, Laboratories, Emergency Medicine, Critical Care, Family Medicine,
Pediatrics, Adolescent Medicine, Internal Medicine, Infectious Disease, Infection
Control Practitioners, Urgent Care, Primary Care Providers, Director of Nursing,
Local Health Departments
New York State Department of Health (NYSDOH), New York City Department of
Health and Mental Hygiene (NYCDOHMH)
HEALTH ADVISORY:
Accelerated Subtyping of Influenza A in Hospitalized Patients
Please see the below Health Advisory from the Centers for Disease Control and
Prevention (CDC) regarding accelerated subtyping for influenza A specimens among
hospitalized individuals testing positive for influenza.
Although the ongoing global outbreak of highly pathogenic avian influenza A(H5N1)
virus has primarily affected dairy cows, poultry, and other animals, 66 human cases
(including one death) have been identified in the United States in 2024. CDC is now
recommending ordering subtyping for all influenza A-positive specimens
collected from hospitalized individuals within 24 hours of hospital admission to
help rapidly detect any human cases of avian influenza A(H5N1).
New York clinicians should:
1. Ask people with suspected or confirmed influenza about potential exposures
to wild and domestic animals, animal products, or symptomatic people with
probable or confirmed avian influenza A(H5).
2. Implement appropriate infection control measures when influenza is
suspected.
o If avian influenza A(H5) is suspected, place the individual in an
airborne infection isolation room (AIIR) with negative pressure, with
standard, contact, and airborne precautions. If none is available, place
a facemask on the individual and isolate in an examination room with
the door closed. The individual should not be placed in any room
where room exhaust is recirculated without high-efficiency particulate
air (HEPA) filtration.
3. Test for influenza A in all hospitalized people with suspected seasonal
influenza or avian influenza A(H5) virus infection, using whatever diagnostic
test is most readily available for initial diagnosis.
o If the initial diagnostic test cannot subtype, order a seasonal
influenza A subtyping diagnostic test within 24 hours of hospital
admission for those who tested positive for influenza A.
• The two main types of seasonal influenza A subtypes are H1
and H3. If a specimen tests positive for one of these subtypes,
H5 testing is not needed, unless exposure history suggests H5
infection.
Seasonal influenza A subtyping tests (e.g., respiratory pathogen
panel with fluA(H1)/(H3) analytes) can be performed in one of
the following settings:
• Hospital clinical laboratory
• Commercial clinical laboratory
• Public health laboratories, if seasonal influenza A
subtyping is not feasible through in-house or commercial
testing.
o If preliminary seasonal influenza subtyping yields an
unsubtypeable result, samples should be promptly submitted to a
public health laboratory for further characterization and potential H5
testing.
o If exposure history or symptoms strongly suggest H5 infection, submit
specimens to a public health laboratory for characterization in lieu of
seasonal subtyping, in line with previous guidance.
o To submit a specimen to a public health laboratory:
For people residing in NYC:
• Send specimens to the NYC Public Health Laboratory for
testing. Call the NYC Health Department’s Public Health
Laboratory at 212-671-5890 to coordinate specimen
submission.
For people residing outside NYC:
• Send specimens to NYS Wadsworth for testing. Specifics
regarding influenza specimen collection and shipping to
Wadsworth Center can be found at:
https://www.wadsworth.org/programs/id/virology/services/
specimen-collection
• A shipping manifest from an electronically submitted
Remote Order OR an Infectious Disease Requisition
(IDR) form requesting influenza testing with subtyping
should accompany all specimens sent to Wadsworth.
• For questions about shipping on holidays or week
New York State is now screening for sub types of influenza a in the appropriate sub group of patients to look for it avian flu. Unfortunately, it now exists in pigs and pig to human transmission is much easier than bird to human transmission. I am assuming that shortly we will have a flu outbreak. I’m concerned about another epidemic and I’m more concerned that the current government has no interest in epidemiology and infection prevention and dealing with a global epidemic.